ORIGINAL ARTICLE | https://doi.org/10.5005/jp-journals-10070-0029 |
Domestic Accidents in the Suburbs of a Metropolitan City in Northern India
1–4Department of Community Medicine, Army College of Medical Sciences, New Delhi, India
Corresponding Author: Gurmeet Kaur, Department of Community Medicine, Army College of Medical Sciences, New Delhi, India, Phone: +91 9953203473, e-mail: drgurmeetkaurkumar@gmail.com
How to cite this article Arora P, Kaur G, et al. Domestic Accidents in the Suburbs of a Metropolitan City in Northern India. J Med Acad 2019;2(1):11–16.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Background: Domestic accidents leading to injuries form a major burden of morbidity in the population. Injuries, like other causes of morbidity, have their own environmental and individual risk factors.
Materials and methods: The study was conducted among 520 individuals belonging to 234 households of a suburban colony of Delhi. Environmental risk factors and occurrence of injuries due to domestic accidents in the last one year of the study were assessed.
Results: The prevalence of injuries was very high in the present study. A total of 418 injuries were reported (803 per 1000 person years). Cuts and falls were the most common injuries. Females, children, and elderly had suffered more injuries.
Conclusion: Most of the households are unsafe and hence the occurrence of injuries is very high. Majority of the injuries were mild and hence preventive education and knowledge for first aid may reduce the burden of injuries in the study population.
Keywords: Domestic accidents, Metropolitan City, Suburbs.
INTRODUCTION
An accident is defined as an unexpected unplanned occurrence that may involve injury. Domestic accidents are unintentional injuries that occur in or around the house.1 Road traffic accidents have been recognized as the leading cause of unintentional injuries, accounting for one-third of the unintentional injuries.2 However, statistics have shown that home injuries too present an important health burden worldwide and the home is a setting that is at least as significant as the road for injury.3
Developing countries, passing through a major epidemiological transition, socio-demographic change, and technological revolution, are facing a triple burden of disease with an unprecedented upsurge of non-communicable diseases and injuries. Recent progress in industrialization and use of vehicles, increased number of people living in crowded and unsafe settlements, coupled with inaccessible and unaffordable emergency health services also contribute to the higher health burden of injuries in the developing regions of the world.4
South-East Asia Region (SEAR), which has 11 low- and middle-income countries, has over a quarter of the world’s total population but comprises about one-third of the world’s unintentional injury-related deaths.5
Home injuries result from a confluence of behavioral, physical, structural, environmental, and social factors,6 illustrating the importance of taking a broad multilevel approach to injury prevention that recognizes reciprocity between the person and the environment, as well as interdependence between points of intervention. The vulnerable populations are children, elderly, and women as they spend most of their time at home and are more at risk in unsafe environments.7
The hazards responsible for injuries at home include unsafe building designs, unsafe furnishings, unsafe packaging and storage of toxic materials, unsafe kitchen, unsafe electrical points unsafe stairs, access to active fire, etc.8–11 For every death, it is estimated that there are dozens of hospitalizations, hundreds of emergency department visits, and thousands of doctors’ appointments apart from many more minor injuries that are not even reported.12 Also, access to services for care and treatment varies widely among population groups. Therefore, hospital-based studies do not give true estimates of the number and pattern of injuries in the community. Most available studies have assessed the burden of injuries only in specific age-groups; so they do not give a true picture of injuries in communities.
Underprivilaged people (living in urban slums, resettlement colonies, and unplanned habitations with unsafe dwelling units and overcrowded living conditions) are especially at risk for domestic accidents.
Therefore, this study was conducted to:
- Ascertain the burden, nature, and severity of injuries due to domestic accidents in people living in a suburban community;
- Assess the environmental risk associated with domestic injuries; and
Thereby, to suggest steps to educate the community regarding the prevention of domestic accidents.
MATERIALS AND METHODS
The study was carried out in Old Nangal Area, Delhi Cantt, the urban field practice area of Department of Community Medicine, ACMS. It is a suburban colony with predominantly people belonging to a low socioeconomic status. The houses are small, multi-storeyed, and unplanned constructions clearly violating the bylaws are rampant.
Sample Size and Data Collection
The unit of study was taken as a household. All individuals, available in the household at the time of data collection, were enrolled in the study.
Studies have reported a varied prevalence of domestic accidents; so taking a prevalence of 13% (as reported from a study from a semi-urban area13) and using the formula 4pq/L2 a margin of error of 5% and design effect of 1.25 (as systematic random sampling was used), the sample size was calculated to be 226.2 (approx. 227).
Old Nangal with an approx. population of 5,000–6,000 has 800–900 households. The first household was selected randomly and thereafter, every 5th household was contacted for data collection. In the case of refusal, the next household was contacted.
A total of 234 households were surveyed and 520 individuals were interviewed. For children younger than 15 years, information was asked from an elder in the house. A pre-designed, pre-tested semi-structured questionnaire was used to record information. The questionnaire consists of the following parts:
- Household questionnaire for sociodemographic information and to assess the environmental risk for domestic injuries (working definitions used for risk assessment are given in Table 1).
- Individual questionnaire to record the number, nature, and severity of injuries due to domestic accidents during the past one year of the survey.
Statistical Analysis
Data collected were coded and analysis was done using SPSS (version 24). Chi-square tests were used to assess the association of factors with injuries among the study subjects. A p value of less than 0.05 has been considered statistically significant.
RESULTS
For most of the risk factors in the physical environment of the households that predispose the inhabitants for injuries (Table 2) (viz. risk for electric shock (66.2%), unsafe kitchen (82.1%), unsafe bathrooms (95.7%), risk because of terrace/staircase (75.7% and 68.8%)), almost two-thirds of the households were unsafe. Unsafe balcony was present in almost half of the houses (47.9%). Many of these households had multiple risk factors for each of these unsafe conditions.
Overcrowding and unsafe storage of chemicals, also risk factors for accidents, were present in almost all (99%) of the households. Most of the households in Nangal were quite unsafe, with the presence of multiple risks in their physical environment. No house was safe, considering the risk factors assessed in the present study.
Almost two-thirds (64%) of the study subjects were in the age group of 16–59 years, 30% were %3C;15 years of age, and 6% were elderly (Table 3). The proportion of males and females was almost equal in the study population. A majority (64%) belonged to joint/extended families (Table 3). Most of the families belonged to lower (75%) or upper-lower socio-economic class as per modified Kuppuswamy classification (updated for 2019).
The occurrence of any injury was found to be significantly associated with extremes of age (Table 4)—that is, in children less than 5 years and elderly more than 60 years (p value—0.006) and also with female gender (p value—0.001). No significant association was found between injuries and type of family or number of family members.
| Risk | Definition |
|---|---|
| Unsafe electric points* | Electric sockets within reach (<3 ft), open wires, wires hanging loose |
| Unsafe kitchen* | Inadequate lighting (inability to read newsprint with max light), wet floor at the time of inspection/inadequate drainage, kitchen within living room, stove on the floor or at height <3 ft, wood/kerosene/coal as fuel |
| Unsafe bathroom* | Presence of wet floor, inadequate drainage, handlebars/railing absent, use of immersion rods without stands and within bathroom |
| Unsafe staircase** | Presence of staircase as risk in itself, staircase without railing, inadequate lighting, unsafe construction (step height %3E;6 inches, width <0.5 m, broken steps) |
| Unsafe balcony** | Presence of balcony as risk in itself, balcony with railing height %3C;3 ft |
| Unsafe terrace** | Presence of terrace as risk in itself, parapet absent/<3 ft height |
| Unsafe storage of chemicals* | Chemicals/medicines accessible to children, chemicals kept near food or water |
* Unsafe if any of the risk factors is present
** Presence of staircase, balcony, terrace is itself a risk
A total of 418 injuries were reported among 520 study subjects in the last one year. Therefore, the average prevalence is 1.24 injuries per person per year due to domestic accidents. The overall prevalence is 803 injuries per 1,000 person years in the study population. The injuries occurred among a total of 357 people, with many people suffering from multiple injuries through the course of last one year of the study.
Overall, considering all injuries sustained, falls were the most common injuries in the study population followed by cuts (Table 5). Other reported injuries were burns, bites by animals, fractures, electric shocks, abrasions, and poisoning (Table 6).
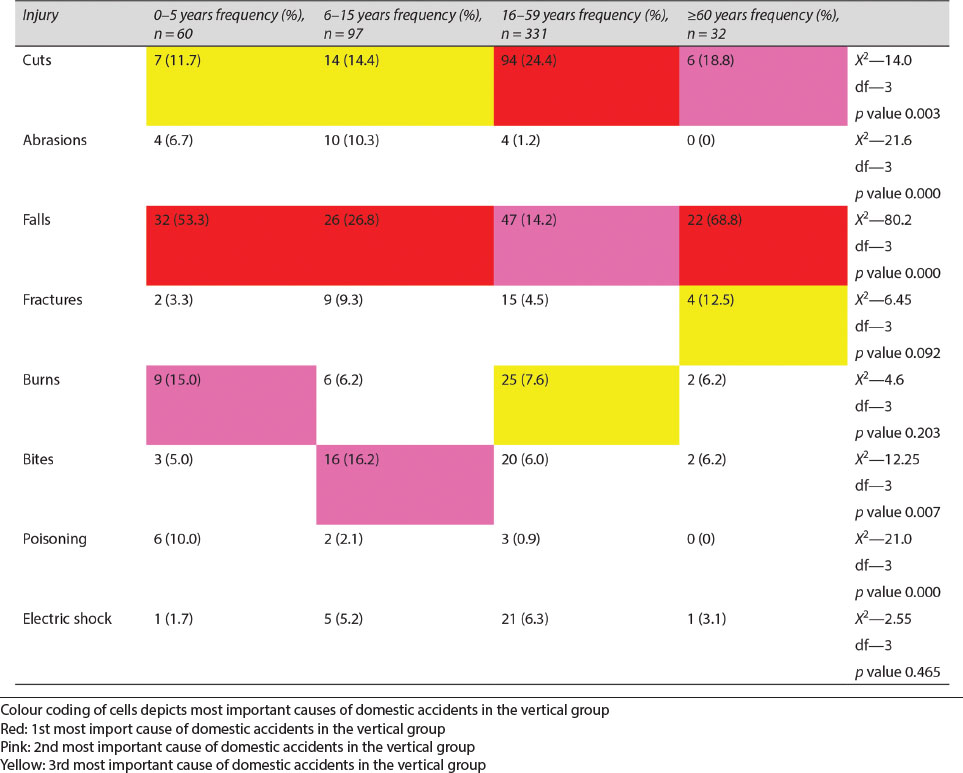
Analysis of specific injuries revealed that a significant association was found between age and occurrence of cuts (more common in 15–59 years; p value—0.003), abrasions (more common in 6–15 years; p value—0.000), falls (more common in elderly; p value—0.000), animals bites (more common in 6–15 years; p value—0.007 and poisoning (more common in children <5 years; p value—0.000)).
Age-wise pattern of all injuries shows that falls were overall the most common injuries sustained in children <15 years of age as well as the elderly aged 60 years or more. In the active age group of 16–59 years, cuts are the most common injuries sustained in the last one year.
Gender-wise analysis of different injuries showed that cuts and burns were significantly more in females (p value 0.000 and 0.006 respectively). Abrasions, fractures, animal bites, and electric shock were more common in males but the difference was not statistically significant.
| Risk | Number | Percentage | |
|---|---|---|---|
| Electric shock risk | |||
| Electric sockets height | Safe | 164 | 70.1 |
| Unsafe | 70 | 29.9 | |
| Open wires | Present | 64 | 27.3 |
| Absent | 170 | 72.7 | |
| Wires hanging loose | Present | 70 | 29.9 |
| Absent | 164 | 70.1 | |
| Number of houses with unsafe electric points—156 (66.2%) | |||
| Kitchen risk | |||
| Lighting | Adequate | 145 | 61.9 |
| Inadequate | 89 | 37.1 | |
| Kitchen within living room | Yes | 111 | 47.4 |
| No | 123 | 52.6 | |
| Wet floor | Yes | 58 | 24.8 |
| No | 176 | 75.2 | |
| Fuel | Lpg | 191 | 81.6 |
| Others | 43 | 18.4 | |
| Stove height | Safe | 163 | 69.6 |
| Unsafe | 71 | 70.4 | |
| Number of houses with unsafe kitchen—192 (82.1%) | |||
| Bathroom risk | |||
| Wet floor | Present | 91 | 38.9 |
| Absent | 143 | 61.1 | |
| Drainage | Satisfactory | 156 | 66.7 |
| Unsatisfactory | 78 | 33.3 | |
| Handle/railing | Present | 38 | 16.2 |
| Absent | 196 | 99.8 | |
| Immersion rod | Unsafe | 102 | 43.6 |
| Safe | 132 | 56.4 | |
| Number of houses with unsafe bathrooms—224 (95.7%) | |||
| Staircase risk | |||
| Railing | Present | 110 | 47.0 |
| Absent | 67 | 28.7 | |
| NA | 57 | 24.3 | |
| Staircase lighting | Adequate | 121 | 51.7 |
| Inadequate | 56 | 24.0 | |
| NA | 57 | 24.3 | |
| Step construction | Safe | 95 | 40.5 |
| Unsafe | 82 | 35.2 | |
| NA | 57 | 24.3 | |
| Number of houses with staircase risk—177 (75.7%) | |||
| Balcony risk | |||
| Railing | Present | 78 | 33.3 |
| Absent | 34 | 14.6 | |
| NA | 122 | 52.1 | |
| Number of houses with balcony risk—112 (47.9%) | |||
| Terrace risk | |||
| Parapet | Present | 119 | 50.8 |
| Absent | 42 | 18.0 | |
| NA | 73 | 31.2 | |
| Number of houses with terrace risk—161 (68.8%) | |||
| Sociodemographic variable | Number | Percentage |
|---|---|---|
| Age (completed years) | ||
| 0–5 | 60 | 11.5 |
| 6–15 | 97 | 18.7 |
| 16–59 | 331 | 63.7 |
| ≥60 | 32 | 6.2 |
| Sex | ||
| Male | 255 | 49.0 |
| Female | 265 | 51.0 |
| Type of family | ||
| Nuclear | 189 | 36.3 |
| Extended/joint | 331 | 63.7 |
| Any injury | No (%) | Yes (%) | X2 (df) | p value |
|---|---|---|---|---|
| Age | ||||
| 0–5 | 18 (30) | 30 (70) | 12.35 (3) | 0.006 |
| 6–15 | 38 (39.2) | 59 (60.8) | ||
| 16–59 | 155 (46.8) | 176 (53.2) | ||
| 60 or older | 7 (21.9) | 25 (71.8) | ||
| Sex | ||||
| Male | 126 (49.4) | 129 (50.6) | 11.52 (1) | 0.001 |
| Female | 92 (34.7) | 173 (64.3) | ||
| Family type | ||||
| Nuclear | 77 (40.7) | 112 (59.3) | 0.170 (1) | 0.680 |
| Joint | 141 (42.6) | 190 (57.4) | ||
| Family size | ||||
| ≤5 members | 72 (39.3) | 111 (60.7) | 0.771 (1) | 0.380 |
| %3E;5 members | 146 (43.3) | 191 (56.7) | ||
The most common injuries among males were falls (22%) and among females were cuts (32.5%). Overall cuts and falls accounted for the majority of burden due to injuries in the study population.
An estimated 87.1% were either treated at home, 11.2% through outpatient consultation and hospitalization beyond 24 hours was required only for 1.7% (7) of the injuries. The injuries that required hospitalization were falls (2), burns (3), animal bite, (1) and fall (1). No deaths occurred in the study population due to domestic accident during the last one year.
DISCUSSION
Household conditions that are risk for accidents (viz. unsafe electric points, unsafe kitchens, and bathrooms) were present in majority of the households. A higher risk (66% vs 90%) for unsafe electric points but lower risk for kitchen (29% vs 82%) when compared to present study have been reported in an urban area of Delhi.9 However, the risk for terrace, balcony, and stairs is lesser in the present study, presumably because lesser number of houses have stairs, balconies, or terraces. The difference could be due to construction and type of houses in the two colonies.
 |
The prevalence of injuries is 1.24 injuries per person per year or 803 injuries per 1,000 person years of observation (80%), which is much higher than that reported in other studies done in urban as well as rural areas of India and also in other developing countries such as Nigeria (the reported prevalence is almost 100 per 1,000 person years).11,12,14–16 However, a high prevalence of 55% has been found in a study done in Pakistan in two communities.7 Higher prevalence (40%) has also been reported by studies done among high-risk groups such as children.9 Most of these studies reporting a lower prevalence have not assessed the risk factors and hence the high occurrence in the present study could be due to the risks in the households in the study area, which are highly unsafe for all parameters assessed. It could also be due to inclusion of all kinds of injuries (including trivial injuries) due to domestic accidents, while other studies have mentioned only specific types of injuries or injuries that cause debilitation for specific time periods.
Most of the injuries occurred in the extremes of age as also reported by other studies.11 However, some studies have reported more injuries in the age group of 15–45 years15–17 probably because the sample consisted of majority of people in this age group in these studies. Also females had more number of injuries as corroborated in other studies as well.7,10,11,13,18 Only Studies that included traffic-related injuries show that number of injuries were more in males.16 This difference was significant across all age groups, thereby highlighting the apathy that females face throughout their life.
Contrary to most other studies that have found injuries to be significantly associated with socioeconomic class and number of family members, this association was not found in the present study presumably because most of the households had similar physical risk factors and overcrowding was present in almost all houses.
Falls, especially in extremes of age (%3C;5 years and %3E;60 years), were the most common injury reported and similar findings have been reported by other studies. However, abrasions were found to have occurred less in the study population when compared to these studies.9,15,16 This could probably be due to the inclusion of injuries in a peridomestic environment in these studies. Cuts were reported as the most common injury among 16- to 59-year-olds and among females, which is consistent with the findings of a study in rural area of Punjab that comprised all age groups.15 Electric shock was more common, while bites and burns were similar to that reported in other studies.9,15
 |
CONCLUSION
The study area is a suburban colony where most people belong to a lower strata of the society. Most of the households in the area are quite unsafe and hence the reported prevalence of domestic injuries is very high in the present study. Cuts and falls account for the major burden of injuries due to domestic accidents. Extremes of age and females are especially vulnerable. Most of the injuries were mild and hence education related to basic safety measures and first aid should be provided to the people so as to enable them to prevent the injuries.
REFERENCES
1. Hogarth J. Glossary of Health Care Terminology, World Health Organisation.Copenhagen; 1978.
2. de Ramirez SS, Hyder AA, et al. Unintentional Injuries: Magnitude, Prevention, and Control. Annu Rev Public Health 2012;33:175–191. DOI: 10.1146/annurev-publhealth-031811-124558 https://doi.org/10.1146/annurev-publhealth-031811-12455.
3. Green LW, Kreuter MW. Evidence hierarchies versus synergistic interventions. Am J Public Health 2010;100:1824–1825. DOI: 10.2105/AJPH.2010.197798.
4. Pant PR, Towner E, et al. Epidemiology of unintentional child injuries in the South-East Asia Region: a systematic review. Int J Inj Contr Saf Promot 2015;22(1):24–32. DOI: 10.1080/17457300.2013.842594.
5. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Global Health Metrics 2018;392(10159):1736–1788.
6. Mack KA, Liller KD, et al. Preventing unintentional injuries in the home using the Health Impact Pyramid. Health Educ Behav 2015;42(1):115S–122S. DOI: 10.1177/1090198114568306.
7. Memon KN, Zeba N, et al. Epidemiologic Patterns of Domestic Accidents and Preventive Measures. Pak Armed Forces Med J 2016;66(5):657–662.
8. Keall MD, Ormandy D, et al. Injuries associated with housing conditions in Europe: a burden of disease study based on 2004 injury data. Environ Health 2011;10:98. DOI: 10.1186/1476-069X-10-98.
9. Bhuvaneswari N, Prasuna JG, et al. An epidemiological study on home injuries among children of 0–14 years in South Delhi. Indian J Public Health 2018;62:4–9.
10. Kommula VM, Kusneniwar GN. A study of domestic accidents in the rural area of South India. Int J Curr Microbiol Appl Sci 2015;4:764–767.
11. Divya BV, Jayasree TM, et al. A study on Occurrence and Risk Factors of Domestic Accidents in South India. Int J Community Med Public Health 2016;3:2387–2392.
12. https://www.who.int/topics/injuries/en/.
13. Stalin P, Senthilvel V, et al. Distribution and impact of domestic accidents in a semi-urban area of coastal Tamil Nadu. India Int J Inj Contr Saf Promot 2015;22(1):11–15. DOI: 10.1080/17457300.2013.835324.
14. Kumarswamy H, Prabhakar VR. Prevalence and Pttern of Domestic Injuries in rural area of Tamil Nadu. Int J Health Allies Sci 2016;5:215–219. DOI: 10.4103/2278-344X.194084.
15. Aggarwal R, Singh G, et al. Pattern Of Domestic Injuries In A Rural Area of India. The Inter J Health 2009;11(2):1–6.
16. Olawale OA, Owoaje ET. Incidence and pattern of injuries among residents of a rural area in SouthWestern Nigeria: a community-based study. BMC Public Health 2007;7:246. DOI: 10.1186/1471-2458-7-246.
17. Mukhopadhya J. A Study of Domestic Accidents (Da) in An Airforce Community. Med J Armed Forces India 1998;54:219–221. DOI: 10.1016/S0377-1237(17)30547-6.
18. Bhanderi DJ, Choudhary S. A study of occurrence of domestic accidents in semi-urban community. Indian J Community Med 2008;33(2):104–106. DOI: 10.4103/0970-0218.40878.
________________________
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.